Symbols of Bipolar Disorder: What They Get Right, What They Get Wrong, and What Actually Matters
July 14, 2026
Is OCD a Disability? Learn when obsessive-compulsive disorder may qualify as a disability, how OCD affects daily life, legal rights, benefits, and treatment options.
Here’s what most people get wrong about OCD:
They think it’s about liking a tidy desk. Alphabetising the spice rack. Being “a bit particular.”
It’s not.
For a lot of people, OCD means hours lost to rituals they can’t stop. Thoughts that hijack their day. A version of daily life that looks nothing like what everyone else takes for granted.
So when someone asks is OCD a disability?, they’re usually not asking out of curiosity. They’re asking because they’re exhausted, because a workplace won’t budge, or because they need to know if the law is actually on their side.
Here’s the honest answer: it depends. Not on the diagnosis itself, but on what the condition actually does to your life. This guide breaks down exactly how that’s decided, under UK law, in the workplace, in schools, and when it comes to benefits. No hype. No guarantees. Just the reality of how disability status actually gets assessed, and what you can do about it.
The Short Answer: It Can Be, Depending on Impact
OCD sits on a spectrum. Some people manage it with a few strategies and get on with their week. Others find it dictates almost everything they do.
Is OCD a disability? In many cases, yes, when the symptoms create substantial, long-term difficulty with everyday life. But not everyone with OCD will meet that bar, legally or otherwise.
Here’s the part that trips people up: it was never really about having OCD. It’s about how much OCD is taking from you, compared to someone without it.
What OCD Actually Is (And What It Isn’t)
Obsessive-Compulsive Disorder is a recognised mental health condition built around two things: obsessions and compulsions.
Everyone double-checks the front door occasionally. Everyone has a preference for how their desk looks. That’s normal, and it’s flexible, it doesn’t run your life.
OCD is different. The thoughts are harder to shut off. The behaviours feel less like a choice and more like a demand. A person with OCD often knows the compulsion doesn’t make logical sense, and does it anyway, because the alternative feels unbearable.
Obsessions: The Thoughts You Didn’t Ask For
Obsessions are intrusive, unwanted thoughts, images, or urges that keep showing up uninvited. They usually bring anxiety, guilt, or plain discomfort with them.
Common patterns include:
- Fear of accidentally harming someone
- Contamination or illness worries
- Relentless fear of making a mistake
- Needing things to feel “just right”
- Intrusive thoughts that clash with a person’s actual values
Here’s something worth repeating: having the thought doesn’t mean wanting it. In OCD, these thoughts are distressing precisely because they go against what the person actually believes.
Compulsions: The Behaviours That Follow
Compulsions are the repetitive actions or mental rituals people use to push the distress back down, or to prevent something bad from happening.
They show up as things like:
- Excessive washing or cleaning
- Repeated checking
- Constantly seeking reassurance
- Counting or silently repeating phrases
- Arranging objects a certain way
- Repeating an action until it “feels” complete
They bring relief. Briefly. Then the cycle resets, and often gets a little stronger each time.
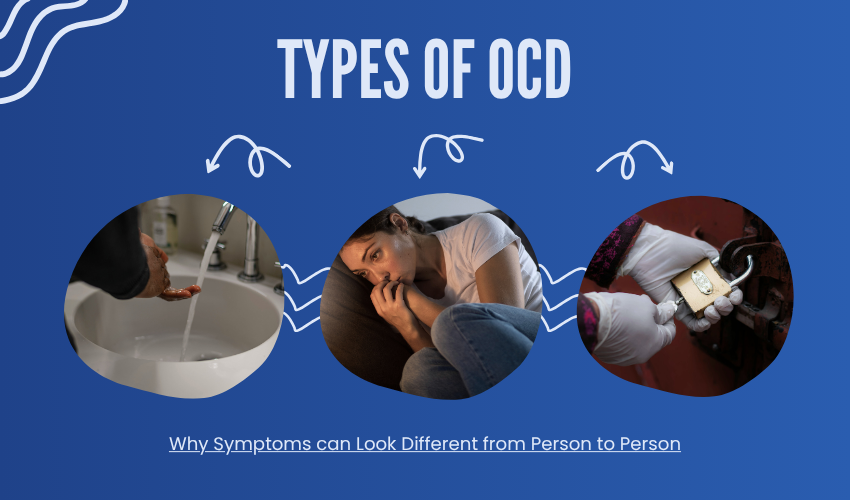
OCD Doesn’t Look the Same Twice
OCD shows up in more forms than people expect:
- Contamination OCD, intense fear of germs or illness
- Checking OCD, repeated checking tied to safety or responsibility
- Harm OCD, fear of accidentally hurting yourself or someone else
- Relationship OCD, persistent doubt about a relationship
- Pure OCD, mostly intrusive thoughts and mental rituals, few visible behaviours
- Symmetry/ordering OCD, a strong pull for things to feel balanced or complete
Two people can carry the same diagnosis and live completely different realities. That’s exactly why functional impact, not the label, does the heavy lifting when it comes to disability.
Is OCD Legally Considered a Disability?
There’s no single, tidy answer here. Disability definitions shift depending on the legal system, the country, and what the assessment is actually for.
Someone might qualify for workplace protection but not financial support. Someone else might need adjustments at university without ever thinking of themselves as “disabled” at all.
The reality: mental health conditions, OCD included, can be recognised as disabilities, but only when they create effects that are both significant and lasting.
How the UK Defines Disability
In the UK, this comes down to the Equality Act 2010.
Under it, someone is considered disabled if they have a physical or mental impairment with a substantial and long-term negative effect on their ability to carry out normal day-to-day activities.
For OCD, that means looking at:
- How severe the symptoms are
- How long they’ve lasted, or are expected to last
- How much they interfere with everyday life
Here’s the part people miss: you don’t need symptoms every single day to meet this definition. It’s the overall impact that counts.
Outside the UK, the Rules Change
Other countries take different approaches, some lean on medical diagnosis, others focus almost entirely on functional limitation.
That distinction affects access to workplace protections, education support, healthcare, and financial assistance. The bottom line: check the specific criteria wherever you are, because assuming the UK rules apply everywhere will only cost you time.
When Does OCD Actually Qualify as a Disability?
Severity and duration are doing most of the work here.
Someone whose OCD is an occasional inconvenience likely isn’t looking at disability recognition. But when symptoms stick around and genuinely restrict daily life, that changes.
Significant impact tends to look like:
- Several hours a day lost to compulsions
- Avoiding important situations because of OCD-driven fear
- Missing work deadlines that would otherwise be manageable
- Distress severe enough to disrupt concentration and decision-making
Where OCD Shows Up in Daily Life
OCD doesn’t stay contained to one part of someone’s life. It can affect:
- Personal care routines
- Leaving the house independently
- Holding down a job
- Completing education
- Building and keeping relationships
- Running a household
Here’s what’s easy to miss: someone can look completely fine on the outside while privately burning hours managing thoughts and rituals nobody else sees.
What Might Meet Disability Criteria
A few real-world examples of where this line gets crossed:
- Someone who can’t work regular hours because compulsions eat several hours daily
- A student who can’t attend class because the anxiety and rituals are too much
- Someone avoiding travel, certain foods, or social contact entirely because of OCD-driven fear
- A person whose relationships are being reshaped by constant reassurance-seeking or avoidance
A professional assessment is what actually confirms the extent of this, not guesswork, not self-diagnosis.
How OCD Plays Out in Real Life
Work and Education
OCD can eat into productivity fast. Excessive checking, rewriting tasks, chasing reassurance, managing intrusive thoughts, all of it takes time that should be going elsewhere.
That can hit:
- Productivity
- Meeting deadlines
- Confidence at work or school
- Career progression
- Attendance and participation
But let’s be clear: OCD doesn’t cap someone’s potential. With the right treatment and support, plenty of people with OCD build strong careers and finish their education without derailing.
Relationships and Family
OCD rarely stays contained to one person. Partners and family members often get pulled into reassurance routines or start accommodating compulsions, usually without realising this keeps the cycle going.
Common friction points:
- Constant need for reassurance
- Avoiding social situations
- Struggling to relax or be spontaneous
- Rising stress across the whole household
Understanding how OCD works helps families respond in ways that actually help, instead of accidentally feeding the problem.
Self-Care and Independence
For more severe cases, ordinary tasks stop being ordinary.
- Showers that stretch on because of contamination fears
- Food preparation derailed by contamination worries
- Struggling to leave the house because of checking rituals
- Avoiding everyday responsibilities altogether
This is where independence quietly erodes, and quality of life along with it.
Emotional Wellbeing
Untreated, severe OCD is exhausting. The cycle of intrusive thoughts, anxiety, and compulsions can bring:
- Ongoing stress
- Low mood
- Social isolation
- Reduced confidence
- Frustration and helplessness
Recognising OCD as a genuine, treatable condition, not a personality quirk, is the first real step toward support.
How OCD Is Actually Assessed
A proper assessment is what separates guesswork from clarity. OCD is typically assessed by a qualified mental health professional, a psychiatrist, clinical psychologist, or another appropriately trained practitioner.
During that assessment, the clinician looks at:
- The nature of the intrusive thoughts and compulsions
- How often symptoms occur
- The level of distress involved
- Time spent managing symptoms
- Impact on work, education, relationships, and daily responsibilities
Here’s the truth: a diagnosis isn’t handed out just because someone has certain thoughts or routines. Most people do, occasionally. What separates OCD is the distress, the loss of control, and the interference with daily functioning.
A thorough assessment can also flag whether something else is contributing, anxiety disorders, depression, or other conditions running alongside it.
The Diagnostic Criteria
Clinicians work from recognised classification systems, the DSM and ICD. Broadly, OCD involves:
- Recurrent obsessions, compulsions, or both
- Symptoms causing real distress or impairment
- Thoughts or behaviours that are hard to control
- Symptoms not better explained by something else
A good clinician weighs the individual’s actual experience, not just a checklist.
Measuring Severity
When it comes to is OCD a disability, functional impact usually carries the most weight. Professionals look at:
- Daily time cost of symptoms
- Whether OCD blocks important activities
- Emotional impact
- Level of avoidance involved
- Whether outside support is needed
Assessment tools help track severity and monitor whether treatment is actually working.
Disability Rights and Reasonable Adjustments
At Work
If OCD meets the legal definition of disability, workplace protections kick in. UK employers carry responsibilities under disability legislation to prevent discrimination and consider reasonable adjustments.
A reasonable adjustment is exactly what it sounds like, a change that removes or reduces the disadvantage someone faces because of their condition.
That might look like:
- Flexible working arrangements
- Adjusted deadlines where appropriate
- A quieter workspace
- Extra breaks when needed
- Supportive conversations with managers or occupational health
What’s needed depends entirely on the role, the symptoms, and the person. Having OCD is not a career ceiling, with understanding and the right support, plenty of people thrive at work.
In Education
Students with OCD may need support too. Severe symptoms can hit concentration, attendance, coursework, and exams.
Support might include:
- Extra time for assessments where appropriate
- Flexibility around attendance
- Access to counselling or wellbeing services
- Adjustments to the learning environment
- Individually tailored support plans
Catching this early means students get help before it derails their education.
Adjustments That Actually Help
- Written instructions to cut down on uncertainty
- Extra preparation time for certain tasks
- Predictable routines wherever possible
- Reducing unnecessary triggers within reason
- Access to mental health support
The goal was never to remove every challenge. It’s to create a fair shot at participating and succeeding.
Can You Claim Disability Benefits for OCD?
Here’s the reality nobody sponsors ads to tell you: a diagnosis alone doesn’t guarantee benefits. Benefit systems look at how a condition affects daily activities and mobility, not the label on a medical record.
In the UK, assessments for support through the Department for Work and Pensions generally focus on practical difficulty with things like:
- Preparing food
- Managing medication or treatment
- Communicating with others
- Making decisions
- Carrying out daily tasks safely
- Travelling independently
Diagnosis Isn’t the Whole Story
Two people can share the exact same diagnosis and live completely different lives. One manages with minimal disruption. The other struggles daily.
Benefit decisions come down to evidence of impairment, how symptoms actually affect independence and functioning, not what the diagnosis says on paper.
What Actually Strengthens an Application
- Reports from psychiatrists, psychologists, or other clinicians
- Treatment records
- Medication history
- Details on symptom frequency
- Concrete examples of everyday difficulty
- Statements from carers, family, or support workers where relevant
Here’s the practical takeaway: keep records. Clear, specific evidence is what actually moves an application forward.
Treatment and Support for OCD
OCD is treatable. That’s not a marketing line, it’s the clinical reality, and it’s worth repeating because so many people assume otherwise.
Psychological Therapy
The leading psychological treatment is Cognitive Behavioural Therapy (CBT), specifically a specialised form called Exposure and Response Prevention (ERP).
ERP involves gradually facing feared situations or thoughts while learning not to lean on compulsions to manage the anxiety.
The goal isn’t to erase every unwanted thought. It’s to build a different relationship with those thoughts, so the compulsion loses its grip.
Medication
Medication comes into play for some people, particularly with moderate to severe symptoms, or when therapy alone hasn’t done enough.
A psychiatrist may discuss options like SSRIs (selective serotonin reuptake inhibitors). This decision should always be personalised, factoring in:
- Symptom severity
- Previous treatments tried
- Possible side effects
- Other health considerations
Self-Management, Alongside Professional Care
Self-help strategies support progress, they don’t replace professional treatment when OCD is genuinely disrupting life.
Useful habits include:
- Learning how OCD actually works
- Practising techniques from a therapist
- Protecting sleep
- Managing stress
- Building supportive relationships
- Resisting the pull to seek constant reassurance
Why Early Action Matters
Left untreated, OCD tends to entrench, avoidance and compulsions become harder to unwind the longer they run. Getting support early gives someone a real shot at learning effective coping strategies before the condition takes more ground.
Here’s the honest picture: OCD can be disabling for some people. It can also be effectively managed for most, with the right treatment in place.
Common Misunderstandings About OCD and Disability
Myth: An OCD Diagnosis Automatically Means “Disabled”
Not true. A diagnosis confirms the condition exists, it doesn’t automatically confirm disability status.
Someone might have intrusive thoughts or occasional compulsions and still work, study, and manage relationships without major disruption. Someone else might lose hours daily to compulsions and struggle to hold down a job.
The diagnosis was never the deciding factor. The impact is.
Myth: OCD Is Just About Cleanliness
Contamination fears and cleaning rituals are one possible pattern, not the whole condition. Plenty of OCD experiences are invisible:
- Distressing intrusive thoughts
- Fear of causing harm
- Excessive doubt
- Mental rituals
- Constant reassurance-seeking
- Fear of making mistakes
These can be just as exhausting as anything visible, often more so, because nobody around the person even knows it’s happening.
Myth: People With OCD Can’t Work or Study
Flatly untrue. OCD says nothing about someone’s intelligence, ability, or potential. Many people with OCD build successful careers and complete their education.
Untreated or severe symptoms can create real friction, but with treatment, understanding, and the right adjustments, most people keep moving toward their goals.
Why Experiences Vary So Much
OCD hits people differently depending on:
- The type of obsessive thoughts involved
- How frequent and intense the compulsions are
- Access to treatment and support
- Personal coping strategies
- Other mental health factors
- The person’s environment
This is exactly why disability considerations come down to the individual, never the diagnosis alone.
When to Seek Professional Help
Signs it might be time to get assessed:
- Significant time lost to compulsions
- Feeling unable to control repetitive thoughts or behaviours
- Avoiding important activities out of fear
- High levels of distress or anxiety
- Work, education, or relationships becoming increasingly difficult
- Leaning heavily on others for reassurance
When OCD starts limiting choices or independence, it’s time to bring in a professional, not push through alone.
Signs symptoms are escalating:
- Old coping strategies stop working
- Compulsions increasing in frequency
- More situations being avoided
- OCD eating up more time each day
- Distress becoming harder to manage
Catching this shift early makes breaking the cycle a lot more achievable.
Where to get support:
- A GP for initial advice and referrals
- A psychiatrist or psychologist specialising in OCD
- Evidence-based psychological therapies
- Mental health services and support organisations
- An online psychiatry assessment, for those who find in-person access difficult
A qualified professional can clarify what’s actually going on, provide a diagnosis where appropriate, and map out treatment options.
Frequently Asked Questions
Is OCD always considered a disability?
No. OCD isn’t automatically a disability in every case. Whether it qualifies depends on symptom severity, how long it’s been affecting the person, and the impact on everyday life. Some people manage symptoms well; others experience impairment significant enough to meet disability criteria.
Can mild OCD qualify as a disability?
Usually not, if it doesn’t substantially affect daily functioning, but every case is assessed individually. What matters is the practical impact of the symptoms, not whether they’re labelled mild, moderate, or severe.
Can you work if you have OCD?
Yes. Many people with OCD build fulfilling, successful careers. Some may need workplace support or reasonable adjustments where symptoms create real difficulty. Treatment, employer understanding, and the right support can make a substantial difference.
Can OCD qualify for disability benefits?
Potentially, yes, if the condition creates significant difficulty with daily living or mobility-related activities. Eligibility comes down to individual circumstances and the evidence provided about functional limitations.
Is OCD recognised under the Equality Act 2010?
It can be, if it meets the legal definition of disability, a substantial and long-term negative effect on someone’s ability to carry out normal day-to-day activities. The diagnosis alone doesn’t settle it; the impact does.
Key Takeaways
Whether OCD is a disability depends entirely on its functional impact. Not the diagnosis. Not the label. How much it’s actually taking from someone’s daily life.
OCD can be genuinely disabling for some people, particularly when intrusive thoughts and compulsions cut into independence, relationships, education, or work.
Legal recognition follows the practical effects, not the diagnosis itself. Severity, duration, and level of impairment are what actually decide legal protection or support eligibility.
OCD is treatable, and support works. Evidence-based therapies, medication where appropriate, and the right adjustments help most people regain control and quality of life. Having OCD doesn’t define anyone’s future, with the right support, most people go on to meet their personal, educational, and professional goals.A professional assessment is the only way to know where you actually stand. If OCD is affecting daily life, that’s the next step, not guesswork, not a checklist online, but a proper clinical evaluation that tells you exactly what’s going on and what to do about it.